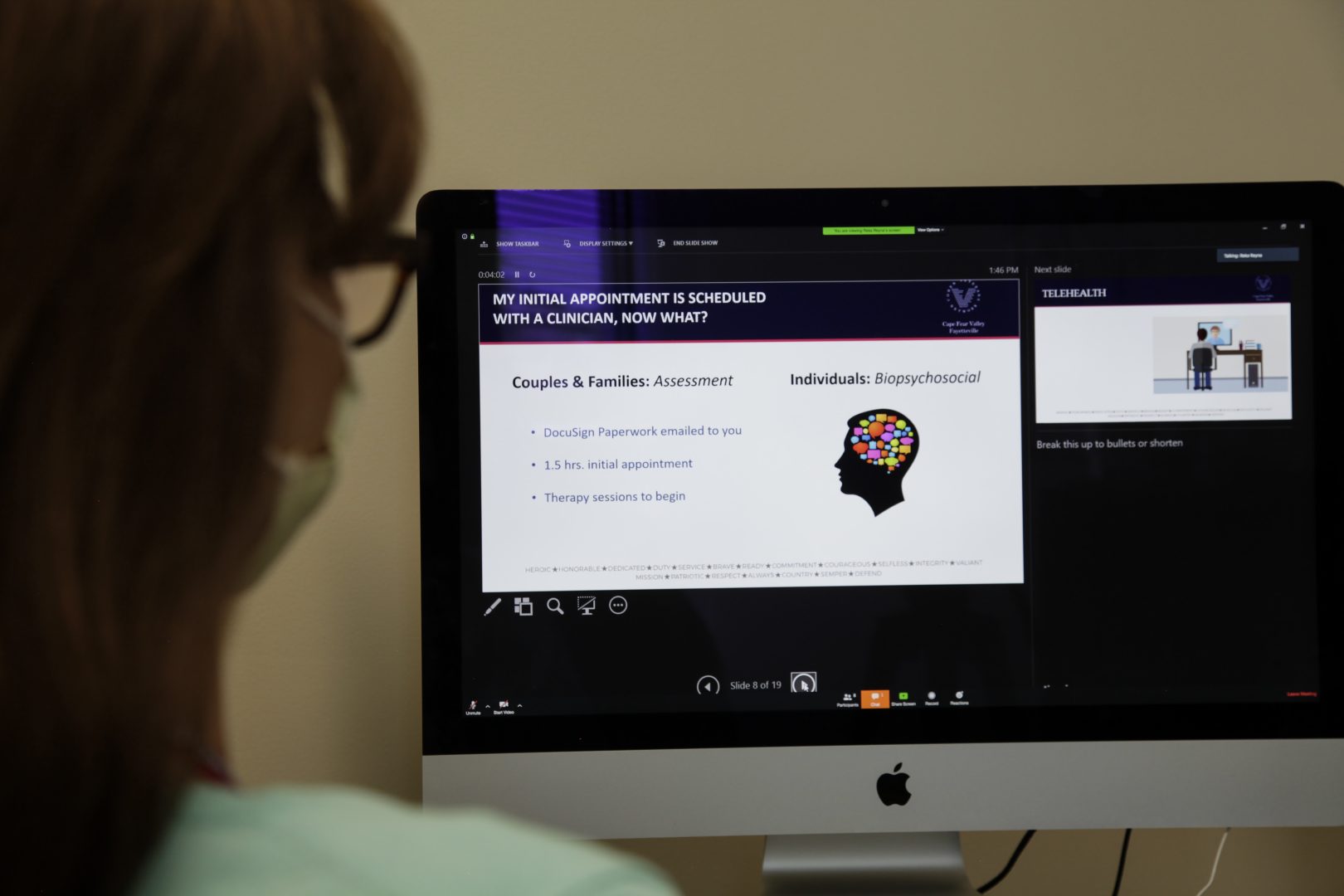
Margo Jarvis takes part in video teleconference at Cohen Veteran's Network's on Wednesday, April 22, 2020, in Fayetteville, N.C.
Sarah Blake Morgan / AP Photo
Margo Jarvis takes part in video teleconference at Cohen Veteran's Network's on Wednesday, April 22, 2020, in Fayetteville, N.C.
Sarah Blake Morgan / AP Photo
Sarah Blake Morgan / AP Photo
Margo Jarvis takes part in video teleconference at Cohen Veteran's Network's on Wednesday, April 22, 2020, in Fayetteville, N.C.
(Philadelphia) — For years, medical researchers have observed stark inequities in the rate of Black patients making it to their primary care appointments after hospitalization. But new research from the University of Pennsylvania shows that the sharp rise in telemedicine appointments during the coronavirus pandemic appears to have eliminated a historical racial health gap in appointment show rates between Black and white patients in a Philadelphia health system.
Prior to the pandemic, use of telemedicine for primary care appointments was rare. The technology was mostly reserved for urgent care visits. But with the onset of the pandemic in March 2020, telemedicine offered the majority of care being delivered, particularly during the mandated shutdowns happening in places such as Philadelphia. Researchers at the University of Pennsylvania wanted to use this period to understand how telemedicine affected access to and quality of medical care in their health system, particularly access to primary care after a major hospitalization.
“And the reason why we chose that setting after hospital discharge is because that’s a particularly vulnerable time for patients, because in that transition period, someone may have been diagnosed with a new condition in the hospital … [or] started brand new medications,” said Srinath Adusumalli, an assistant professor of clinical medicine in cardiology, assistant chief medical information officer of connected health strategy and applications, and the study’s senior author.

LM Otero / AP Photo
Medical director of Doctor on Demand Dr. Vibin Roy prepares to conduct an online visit with a patient from his work station at home, April 23, 2021, in Keller, Texas.
Pulled for the study was data from five Penn Medicine hospitals in Philadelphia on post-hospitalization primary care follow-up appointments from 2019 through 2021. What Adusumalli and his team found was that telemedicine visits in general were associated with improved markers of access, including decreased time to follow-up for an appointment after hospital discharge, and increased completion of post-hospital follow-up discharge visits.
Overall, patients in the study population experienced boosts in access to care through the increased availability of telemedicine. Post-discharge primary care visit completion rates climbed from 62% to 72% from January to June 2020. But one of the most significant boosts was observed for Black patients, highlighting telemedicine’s potential for bridging long-standing health inequities.
According to Adusumalli, preexisting inequities for appointment completion rates between Black and white patients have long been observed. But data from this study shows that widespread access to telehealth increased Black patients’ visit completion rates to 70%, from 52%. For white patients, by contrast, there was little change, from 68% in January 2020 to 67% in June 2020.
Researchers hypothesize that one of the reasons telemedicine may be closing some of these racial health gaps is because it makes appointments more convenient and brings care closer to where a patient is. Physically traveling to a clinic, taking time off work — particularly when you’re recovering from a recent hospitalization — are just some of the many difficulties that present barriers for patients to follow-up care.
Dr. Eric Bressman is the study’s lead author, a fellow in the National Clinician Scholars Program, and an internist at Penn Medicine. He noted that for Black patients specifically, there are long-documented racial disparities in geographic access to clinics.
“There were greater barriers to geographic access to primary care for Black patients than for white patients,” Bressman said. “And when you start to think about the advantages that telemedicine confers, you can see how it might level the playing field in terms of access to care. For white patients, the attendance rate to postdischarge trial appointments remained just about the same [during a period of increased access to telehealth]. But for Black patients, it jumped 15 to 20 percentage points, which was kind of astounding.”
The boost the researchers documented effectively eliminated the historical racial gap in show rates to follow-up appointments. But Bressman and Adusumalli said many questions remain about the viability of telemedicine. One such concern has to do with the quality of care that is delivered through telehealth. Researchers say that there can be a range in the quality of various telemedicine tools — and that studying that can present challenges because of the self-reporting bias reflected in who chooses to opt into telemedicine.
“How does [telehealth] improve the recovery after hospital discharge? What does that mean for the likelihood that they’re going to be readmitted to the hospital within 30 days, and what does it mean for their overall recovery? All of those questions remain unanswered,” Bressman said.

Courtesy of Aditi Joshi
Dr. Aditi Joshi, director of JeffConnect, Thomas Jefferson University Hospital’s telehealth platform, opens EPIC, the hospital’s electronic medical records program. That way she can look up at patient’s history and see scans and other test results before meeting with them virtually.
Telehealth also presents challenges to the delivery of care. Access to the technology required to have a telehealth appointment is a huge issue. There are significant disparities in access to broadband internet, cellphones, and computers. In addition, the physical markers of poor health doctors can observe during in-person visits become a lot more challenging to see during remote appointments.
“From a visual perspective, there’s a lot you can learn from examining a patient visually,” said Adusumalli. “How fast are they breathing? You can look at their veins in their neck, for example, to see [if] they have extra fluid on their body.”
But there are a range of new devices, some of which are being piloted at Penn Medicine, that aim to address that challenge in care for telehealth delivery. These range from devices that allow doctors to see inside a patient’s nose, mouth, and throat, to devices that can allow doctors to listen to lung and heart sounds remotely. Other peripheral devices, such as scales and blood pressure cuffs, can bring information directly to doctors that they otherwise would not have access to virtually.
And, according to Adusumalli, the experience of administering remote care in a person’s home environment rather than the traditional doctor’s office or hospital creates some positive gains.
“It’s so valuable … to see a patient at home in their environment because we never really have that opportunity to interact with a patient in that way, where perhaps they’re a bit more comfortable,” said Adusumalli. “And you can actually see how they take their medications every day, what the home environment looks like. All of that gives you such a richer picture potentially of a patient’s health than an office visit.”
The future of telemedicine is precarious. During the pandemic, much of telemedicine across the country has been enabled by waivers that mandated insurers to cover those services and enabled providers to deliver care across state lines. But Bressman said a lot of those waivers are starting to expire. And policymakers across the United States are scrambling to determine how to make access to telemedicine available for years to come.
“We’re trying to understand what the impact of those waiver expirations will be and how policymakers [will] map out which of those waivers they should carry forward to continue to keep this service available for patients, because it was and continues to be a vital access point,” said Bressman.
The field is still a relatively new one, and Adusumalli said further research is needed to understand its full impact on patients, clinicians, and health care delivery systems: What are the qualitative experiences of doctors and patients who use telehealth? How does the management of certain conditions differ for patients using telemedicine versus patients seeking care in in-person settings? Those are questions researchers want to be able to answer in the coming years.
“We’re very excited to be able to … contribute to closing historic inequities in access to care using digital channels,” said Adusumalli. “I think what will be important as we continue to go forward is to make this really a guiding principle and a high priority for the design and development of our fellow medical health system.”

A collection of interviews, photos, and music videos, featuring local musicians who have stopped by the WITF performance studio to share a little discussion and sound. Produced by WITF’s Joe Ulrich.